
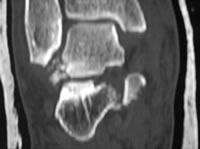
Comminuted fracture of lateral talar process (type 3) with rotated fracture of the sustentaculum medially - presumably a self-reduced subtalar dislocation
The lateral process is the attachment of the lateral talocalcaneal ligament and the subtalar joint capsule. Fractures of the process are due to axial loading of a dorsiflexed ankle, especially with eversion (Funk 2003, von Knoch 2007). It is particularly associated with snowboarding injuries, hence the name “snowboarder’s ankle”. Kirkpatrick et al (1998) found that lateral process fractures accounted for 15% of ankle injuries in a large study of snowboarding injuries. Indeed, almost all published cases occurred in snowboarders, although Hawkins' (1965) original series mostly resulted from motor accidents and falls, and the authors have seen them in low-energy falls.
von Knoch et al (2007) drew attention to the high incidence of associated injuries such as calcaneofibular ligament tears, peroneal tendon sheath tears and chondral injuries to the calcaneal facet of the subtalar joint.
Clinical features
Clinically a fracture of the lateral talar process has the same appearance as a major lateral ligament injury of the ankle – lateral pain, swelling and bruising. Hence it tends to be an incidental finding at radiography of an injured ankle which is failing to settle, and is often missed initially (Kirkpatrick 1998). The presence of such a picture after a snowboarding injury should certainly arouse suspicion.
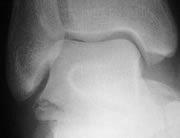
A fracture of the process disrupts the "V" shape

The lateral process normally makes a distinct "V" shape on the lateral radiograph
von Knoch et al(2007)'s V-sign
Imaging and classification
The injury may be overlooked on plain radiographs. von Knoch et al (2007) described a "V-sign" on lateral radiographs: the lateral process normally makes a distinct "V" shape and disruption or displacement of this suggests lateral process fracture. Plain radiography may underestimate the size and significance of the fragment. Broden views or CT are useful if there is a possible intention to fix the fracture. Arthroscopy allows assessment of the subtalar joint, and can be used to assess fracture reduction.
The original classification was by Hawkins:
- simple fracture involving both subtalar and ankle joints
- comminuted fracture
- "chip" fracture

CT shows the full size, but the joint surface is non-comminuted
Intermediate-sized articular fragment - type 2 (snowboarder)
McCrory and Bladin et al (1996) proposed:
- single small fragment involving ankle and subtalar joints
- single large fragment involving ankle and subtalar joints (sometimes carrying a substantial proportion of the subtalar joint surface)
- comminuted fracture
and this was used by both the largest series (Valderrabano et al 2005, von Knoch et al 2007). The majority of fractures (16/20 in Valderrabano's series and 15/23 in von Knoch's) were type 2.
Management
Most series treated McCrory-Bladin type 1 fractures with splintage and partial weightbearing. Both Valderrabano and von Knoch treated the majority of type 2 fractures surgically, mostly fixing with two small screws. von Knoch operated on 5/7 of type 3 fractures, using bone graft and small buttress plates where necessary.
Valderrabano reported significantly better AOFAS hindfoot scores in the surgically treated patients, but von Knoch found a small (probably non-significant) advantage for the non-surgically treated patients. More of von Knoch's operated patients had comminuted fractures, which did worse, so their results may reflect case mix rather than surgical results alone.
Most series report about 15% late subtalar arthritis, although von Knoch reported 43%, which might, again, reflect case-mix.
There have been no controlled trials of treatment, which mainly reflects the rarity of the injury.
References
- Funk JR et al. Snowboarder's talus fractures experimentally produced by eversion and dorsiflexion. Am J Sports Med 2003; 31:921-8
- Hawkins LG. Fracture of the lateral process of the talus. JBJS 1965; 47A:1170-5
- Kirkpatrick DP et al. The snowboarder's foot and ankle. Am J Sports Med 1998; 26:271-7
- McCrory P, Bladin C. Fractures of the lateral process of the talus: a clinical review. "Snowboarder's ankle". Clin J Sports Med 1996; 6:124-8
- Valderrabano V et al. Snowboarder's talus fracture:treatment outcomes of 20 cases after 3.5 years. Am J Sports Med 2005; 33:871-80
- von Knoch F et al. Fracture of the lateral process of the talus in snowboarders. JBJS 2007; 89B:772-7