
A recent systematic review of Charcot neuroarthropathy was authored by Rogers (2011) on behalf of the American Podiatric Medical Association and the American Diabetes Association. Other good reviews include Schade (2015) and Idosuyi (2015).
Patients who have had Charcot arthropathy will often be left with bony deformitywhich may be stiff (midfoot) or unstable (peritalar, ankle or hindfoot). There is often fixed hindfoot equinus. These deformities increase the pressures under the midfoot and increase the risk of recurrent ulceration.
Many patients can be satisfactorily managed in accommodative shoes and total contact moulded orthoses. However, a proportion of patients will have persistent or recurrent ulceration despite optimal orthotic management. Pinzur (2004) carried out realignment or exostectomy in 41% of 147 Charcot feet with midfoot involvement because of inability to achive satisfactory orthotic fitting, although it is not clear how many of these pateints had recurrent ulceration. In Saltzmann's (2005) series, 49% had at least one ulcer, 28% recurrent ulceration, 9% had excision of bony prominences and 12% trans-tibial amputation.
The patient’s overall condition should be optimised, infection controlled and ulceration healed if possible. The main surgical options are:
Exostectomy
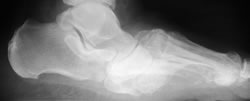
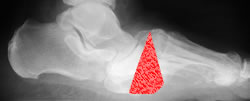
Plantar bony prominences can be excised through a longitudinal medial and/or lateral incision. Provided the foot is stable, ulcer healing is achieved in 74-91% of patients (Brodsky + Rouse 1993, Catanzariti 2000, Pinzur et al 2004, Saltzmann 2005, Laurinaviciene 2008). However, there may be continuing collapse in the foot or the amount of resection may lead to instability. We have had one recurrence, in a patient who had some residual midfoot instability, but he preferred repeat exostectomy, which resulted in stable healing.



A large plantar bony prominence with recurrent ulceration was excised giving an easily accommodated deformity
Corrective osteotomy/fusion
Correction of deformity by midfoot osteotomy-fusion, triple fusion or tibio-talo-calcaneal fusion, depending on the level of deformity has been described by Schon et al (1998), Sammarco and Conti (1998), Pinzur et al (2004), Saltzmann (2005) and Grant (2009). Lowery (2012) reported a systematic review of surgery for Charcot. In 246 reported patients, 76% achieved bony fusion, 22% fibrous or non-union and 1.2% underwent amputation. Most non-unions are sufficiently stable to allow mobilisation with bracing.
Surgery in the presence of unhealed ulceration or infection increases the risks greatly. However, Early and Hansen (1996) managed to achieve fusion in 19 of 21 feet and ulcer healing in 7 of 10 ulcers, with two amputations for osteomyelitis.




Severe Charcot deformity corrected with biplanar closing wedge osteotomy and double plate fixation
Amputation
Trans-tibial amputation is usually preferred, as prosthetic fitting is easier. However, hindfoot amputations such as the Syme procedure allow weightbearing mobilisation on the stump, which can be useful for patients with generally poor mobility and often poor eyesight. Pinzur (2003) achieved mobility with a prosthesis in 80/82 diabetic patients, although it is not stated how many of these had Charcot arthropathy.